Welcome to April and my favourite time of the year – Autumn.
No, I wasn’t going to say “footy season”. I don’t get to the football much these days but living in a family of ardent Collingwood supporters means it is pretty much all I hear about from now until September.
The football season I’m most familiar with is the one we have at Melbourne Hand Therapy. It’s a busy time of year for us as we see players big and small (and sometimes tiny) whose hands, fingers, elbows and shoulders manage to get caught up in the rough and tumble of the game. Even the Auskick preppies find ways to land awkwardly on their elbows.
For the past couple of weeks, we have run a series of articles on social media highlighting the most common football injuries that come through our door. We have tried to be as reassuring as possible so players know that, with the right therapy, they will return to the game. Just to recap, the most common football injuries we see at Melbourne Hand Therapy are dislocated shoulders, broken collarbones, elbows which have been hyperextended and damage to the ligaments around the bone that joins the arm to the elbow. You can read about them below.
In March, I joined MHT physiotherapist Dane Johnson to deliver an intermediate-level course for the Occupational Therapy Association on how to assess common hand conditions. We were really focusing on the critical skills needed by therapists to diagnose a patient’s condition and to develop an effective treatment plan, which includes – crucially – knowing when to call in a surgeon. We had a great time and really want to thank those who participated.
We also welcomed a new member to the MHT family, Vanessa. Vanessa will be working as a receptionist at our Ringwood clinic on Fridays. Look out for her if you have appointments with Kim, Nikita or Rose.
In this newsletter we will also be focusing on Complex Regional Pain Syndrome – a chronic and debilitating syndrome for patients and one of the most challenging conditions for therapists to diagnose and treat.
Have a lovely April and, for the sake of my winter peace, go Collingwood!
FOOTY’S BACK BUT SO TOO ARE THE INJURIES
For the past couple of weeks, we have run a series of articles on social media highlighting the most common football injuries that come through our door. We have tried to be as reassuring as possible so players (and their long-suffering mums) know that, with the right therapy, they will recover and return to the game. Just to recap, the most common football injuries we see at Melbourne Hand Therapy are dislocated shoulders, broken collarbones, elbows which have been hyperextended and damage to the ligaments around the bone that joins the arm to the elbow.
An anterior dislocation occurs during high intensity tackles where the shoulder is forcefully pushed to the side and rotated, resulting in dislocation. Therapy involves examination of the shoulder, scans, immobilization and a variety of exercises and generally requires our male and female footballers to remain on the sideline for a period of time. It’s a frustrating injury but players do recover and confidently return to the game.
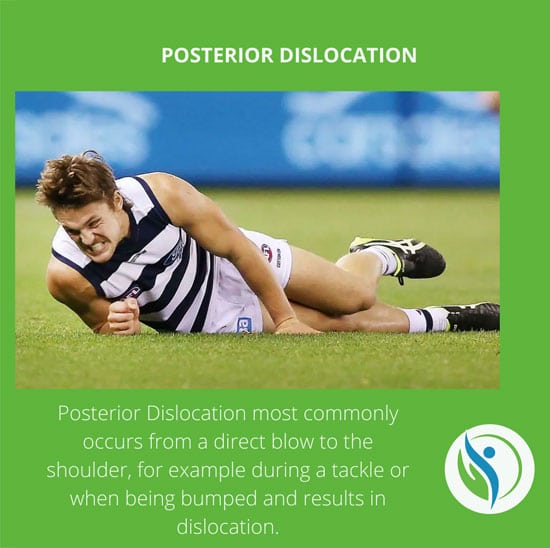
A very rare condition compared to the anterior dislocation, a posterior dislocation most commonly occurs from a direct blow to the shoulder and occurs when players bump each other when competing for the ball, either in a tackle, a marking situation or in a scuffle on the ground. It can be painful but first needs an accurate diagnosis by doing scans and relocation of the shoulder, a period of rest and exercises players can be back in the thick of it within 12 weeks.
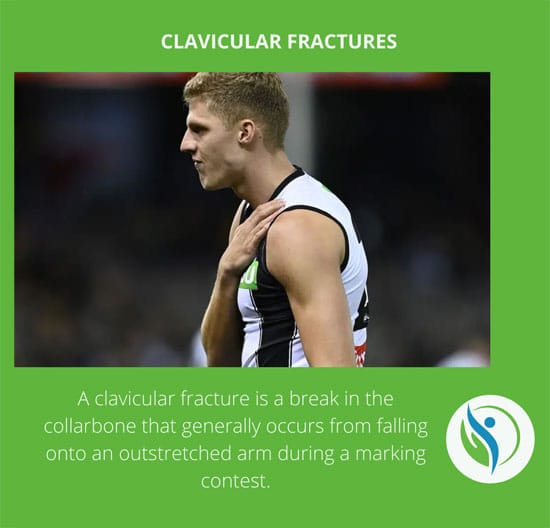
A clavicular fracture is a painful break of the bone that connects the breastbone to the shoulder. It generally occurs when a player falls onto the tip of the shoulder or a marking contest. Treatment generally involves a period of resting and avoiding loading but gentle movement. Depending on the severity of the fracture, players can expect to be on the sidelines for 10-12 weeks.
AC – or Aromioclavicular – joint sprains are common and usually result from a fall on the shoulder, a fall on an outstretched arm or a solid bump to the shoulder. The injury occurs to the strong ligaments that join the shoulder to the collarbone and can range from a relatively minor injury like a sprain to very serious injury where all the stabilising ligaments are ruptured. A sprain can see a player sidelines for a couple of weeks while a serious rupture can result in surgery and a season-long recovery.
Hyperextension of the elbow is an injury we see a lot of at MHT during the football season and it occurs when the elbow is bent back away from its natural angle. This seems to happen more often than not during a tackle or a fall. Depending on the severity of the damage, treatment is different and can include a period of rest, an ice pack, elevation and compression. As soon as the symptoms settle, down exercises can start. In a very serious injury, surgery is required. Depending on the severity of the injury, a player can expect to be back in the thick of the game within 12 – 16 weeks.
Complex regional pain syndrome (CRPS) is probably one of the most challenging conditions we at Melbourne Hand Therapy see. This is because the degree of pain suffered by a patient is not always obvious to the clinician involved. Also, the pain might not be proportional to the size of the injury. Often, a minor trauma can cause a higher-than-expected degree of pain.
Pain is the body’s way of protecting us and it is real. It is important our patients know this and know that at Melbourne Hand Therapy, we understand this. Pain is a necessary part of human development. It is an automatic reaction by the body to let us know we are doing something harmful and have to stop.
60 per cent of CRPS cases present in the upper limb compared to 40% in the lower limb. In the case of distal radius fractures – fractures of the wrist – the incidence of CRPS ranges from one to 37 per cent.
Melbourne Hand Therapy uses the Budapest Criteria to diagnose CRPS. This scale assesses the symptoms of CRPS based on several factors. Firstly, we assess symptoms based on sensory changes which relate to changes in pain sensitivity in the patient. Secondly, we evaluate vasomotor changes. This refers to the changes in the diameter of blood vessels during the natural processes of contraction and expansion of the blood vessels known as vasodilation and vasoconstriction. Thirdly, we look at the patient’s sudomotor reaction which refers mostly to the degree to which a patient is sweating even in the absence of exertion or intense physical activity. Finally, we look at the motor or trophic changes, or limitations of movement.
There are two types of CRPS. Type one occurs after trauma and causes sensory, motor, automatic and skin/bone changes. Type two includes all these changes plus the involvement of nerves.
Treatment for CRPS includes upper limb therapy often in conjunction with pharmacological treatment (such as pain medication). At Melbourne Hand Therapy, our treatment also involves patient education and a customised graded motor imagery program.
Graded motor imagery consists of laterality (left/right discrimination), imagined movements and mirror therapy. It is a well-researched field by Mr David Butler and Mr Lorimer Moseley etc al. We utilise this research in our clinical practice and often share textbooks, apps, mirrors and flashcards as part of our treatment approach.
EDUCATION
When patients present at Melbourne Hand Therapy in a state of chronic pain, we know that in reality, they will only be with us for a very short period (0.1% of the time). In that short period, we endeavour to equip them with all the skills they need to become an integral part of the management of their own injury and recovery, and to enable them to have the confidence to be critical thinkers and problem-solvers in the treatment and healing process.
Biopsychosocial Model
When attempting to diagnose the level of pain, Melbourne Hand Therapy uses the biopsychosocial model. This model has three interacting components – bio, psycho and social. The biological factors consider the patient’s genetics and the health of the tissue surrounding the injury. The psychosocial factors consider all that makes us human – such as our knowledge, thoughts and emotions. Lastly, we take into account social factors which include our relationships, communities and culture.
At Melbourne Hand Therapy, our focus is to provide pain biology education with a customised movement approach to increase our patient’s physical capacity, reduce their pain and improve their quality of life. It is important that our patients understand that movement is beneficial, but of course in a graded, gentle way. This is called graded exposure, also known as “pacing”.
WELCOME VANESSA TO THE MHT FAMILY.
We are so excited to welcome Vanessa who will be working in our Ringwood clinic every Friday. Vanessa has a background as a naturopath and has worked as a receptionist for the last ten years. She works four days a week at Precision Gastro which she plans to continue but will be all ours on Fridays to support Kim, Nikita and Rose. So pop into MHT’s Ringwood practice at 176 Mt Dandenong Rd and say “hello”.
FAST FIVE WITH KIM
1) What football team do you support and why? Although I am from Scotland I have really enjoyed watching the AFL since I moved here and support the Richmond Tigers. Most people think that I chose to support them because they had just won the Premiership the year before I arrived in Melbourne but I actually didn’t know that they were the reigning Premiers and just decided to support them because I live in Richmond and wanted to support the local team!
2) What are you reading at the moment? I am part of a book club so this month’s book that I am currently reading is ‘Daddy’ by Emily Cline.
3) What is your guilty streaming pleasure? Oh I have a few. I have just spent the last few days binge watching the latest season of ‘Drive to Survive’ on Netflix which I love. When there is nothing else, I like to rewatch old comedy series such as Brooklyn 99 or The Big Bang Theory.
4) What do you do to relax? A wine with some friends is always the best way to relax in my opinion.
5) What was your first job? My first job was working in a deli in a supermarket in Scotland called Somerfields. They went bust a couple of years ago.